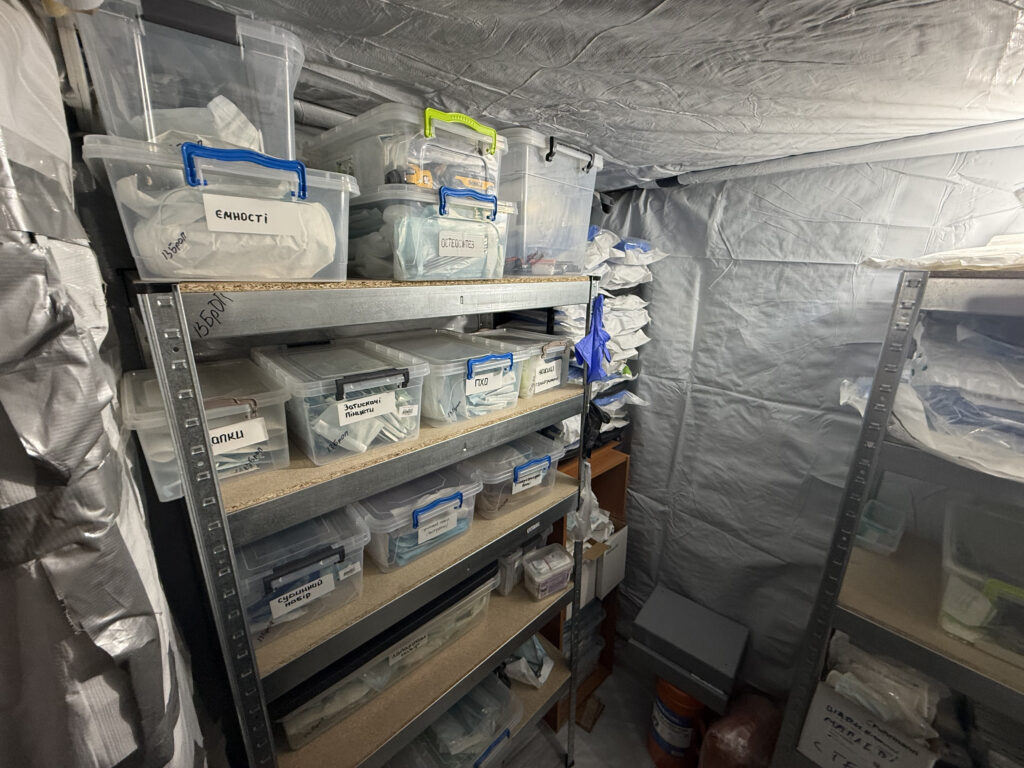
Our team visited a stabilization point near the front line — less than 20 kilometers from active combat zones. This is where wounded soldiers are brought after evacuation, and where medics work in a reality where only minutes often stand between life and death. We spoke with a surgeon, an anesthesiologist, and the medical team working there every day about what a stabilization point really looks like from the inside, why time remains the greatest challenge of this war, how telemedicine is saving lives under fire, and what the phrase “the golden hour” truly means on the modern battlefield.
Time That Does Not Exist: Evacuation and the Limits of Medicine
A stabilization point in war is not a hospital in the usual sense, nor simply an intermediate link between the battlefield and a hospital. It is a place where medicine functions under conditions in which time has already been lost — or nearly lost — and decisions must be made faster than normal human psychology allows. It is here that a wounded soldier who has been evacuated from the battlefield first reaches a team capable not only of stopping critical bleeding or relieving pain, but of stabilizing the patient enough to survive the next stage — transport, surgery, hospitalization, rehabilitation.
Anesthesiologist Dmytro, who works at a stabilization point, speaks about his work without romanticizing it. There is no pathos in his words, although the reality he describes is stronger than any pathos. What troubles him most is not the complexity of injuries or the exhaustion of the team, but the fact that sometimes wounded soldiers cannot be evacuated from the battlefield in time. “The thing that upsets me the most is the inability to evacuate a wounded person from the battlefield in time,” he explains. “We know the person is wounded, we are ready, we have the conditions necessary to provide care, but sometimes evacuation from the battlefield either takes a very long time or does not happen at all.”

Military medicine often speaks about the “golden hour” — the critical period after injury during which the chance of survival is highest. But in this war, especially on certain sections of the front line, that formula does not always work. The doctor describes it almost bitterly: “As they say — the golden hour. For us, it’s a golden week.” There were cases when wounded soldiers remained in positions for too long, while medics could support them only remotely: dropping antibiotics by drone, consulting on what medications to administer, how to dilute them, what to do until evacuation became possible.
This is where one of the key realities of modern frontline medicine becomes visible: the problem is not always the absence of specialists, medications, or skills. Very often, the problem is that between the wounded soldier and the doctor lies the battlefield itself — drones, artillery, destroyed roads, weather, the absence of safe evacuation routes, and constant danger for evacuation teams. That is why a stabilization point works not only with the wounded body, but also with the consequences of delays that medicine itself cannot control.
Under these conditions, telemedicine stops being a modern buzzword from presentations and becomes a practical survival tool. Doctors consult combat medics and soldiers remotely, sometimes effectively directing care in real time. “We called and explained what to do: how to bandage, where to apply pressure, where to pack the wound,” recalls surgeon Yevhen. In one case, according to him, remote guidance made it possible to remove tourniquets, control bleeding, and save a limb. This does not replace evacuation and does not eliminate the need for surgery, but sometimes such remote support gives a person a chance to survive until help arrives.

Working at the Edge: Stabilization, Decisions, and Responsibility
When the wounded finally arrive at the stabilization point, the team must act quickly, but not mechanically. Stabilization is not a chaotic set of actions, nor an automatic process of “stitching someone up and sending them onward.” It is a complex process in which every step depends on the patient’s condition: whether the person is in shock, hypothermic, suffering from massive blood loss, whether blood pressure is stable, whether the body can tolerate intervention. “A soldier arrives soaked, cold, without pain management. He has to be undressed, laid down, dried off, warmed up, provided with anesthesiology support, stabilized in terms of blood pressure and other indicators. Only then can the surgical team work safely,” explains surgeon Yevhen.
That is why the amount of time spent at a stabilization point cannot fit into a single chart. If the patient is relatively stable, treatment may take 15–20 minutes. If the condition is severe, doctors may work for two or three hours. To civilians, that may sound like a long time, but for frontline medicine it is sometimes the only opportunity not to lose the patient before reaching the hospital. “Medicine is not always two plus two,” says the surgeon. “Everything depends on the patient’s condition, the extent of the injury, the amount of care required, and the stabilization measures needed.”

A particularly difficult topic is amputations and severe limb injuries. According to the doctor, stabilization points are not places for “planned” amputations in the hospital sense. If a limb is nonviable, the team does not attempt to make a final decision in conditions where not all capabilities are available. Their task is to stabilize the patient, avoid worsening the condition, preserve whatever may matter for future surgical work and prosthetics, and transfer the patient to the next level of care. “The hospital shapes the residual limb in a way that is more adapted for prosthetics,” explains Yevhen. “If we see that the limb is nonviable, we do not remove the tourniquet, we perform surgical debridement, stabilize the patient, and prepare them for transport.”
This is important to understand: a stabilization point is not a place of “final treatment.” It is a place where a wounded person must be moved from a state of catastrophe into a condition in which transport becomes possible. The patient’s story is not completed there — they are given a chance for it to continue. In this sense, the anesthesiologist’s role is one of the central ones: not simply “administering anesthesia,” but guiding the patient through the most dangerous interval — between uncontrolled post-traumatic condition and the possibility of surgical intervention.
War constantly destroys any sterile image of medicine. Patients may arrive on ATVs, improvised stretchers, covered in mud, soaked, freezing, after prolonged periods in frontline positions. The doctor recalls cases when a wounded soldier essentially “flew into” the stabilization point in a condition where only the eyes were visible, while everything else — mud, clothing, blood, exhaustion — blended together. The team cuts away clothing, pulls the person out, evaluates the condition, and starts working. This is the daily reality in which stabilization points exist: not under ideal protocols, but under the conditions of war, where every case brings a different scenario.
Impact and Systemic Change: From Experience to Standards
Despite this, medics speak not only about survival, but also about development. One of the recurring requests in these conversations is for more opportunities for training, professional exchange, conferences, workshops, and courses. This is not a “bonus” or abstract self-education. For people who work every day with the harshest consequences of war, development means better decisions, fewer mistakes, faster responses, and a greater chance of survival for patients. The conversation directly mentions the need for funding conferences, courses, visiting workshops, and exchanges with specialists.
Already in Ukraine, several educational initiatives are being launched or discussed: the ASET course, the future implementation of ATLS, work related to infection control, and educational initiatives connected to Razom Health. It is separately emphasized that infections in hospitals have become such a serious problem that they require an entire direction of work on their own. This is another indication that frontline medicine does not end at stabilization. A wounded person moves through a long chain, and the quality of every stage affects the outcome: from first aid at the position to evacuation, stabilization points, hospitals, infection control, rehabilitation, and return to life.
In this context, the Razom Heroes program plays a key role, working not with isolated cases but with the system as a whole. This includes the training of combat medics and instructors, equipping units, developing educational programs, and creating conditions in which frontline experience does not remain at the level of isolated stories, but is transformed into standards. It is through programs like these that a connection is formed between the reality of stabilization points and long-term systemic change: implementation of training courses, development of telemedicine, support for instructor programs, systematization of knowledge, and transfer of that knowledge to other units.
A stabilization point is a place where medicine looks least like a beautiful story and most like a struggle against time. Not everyone can always be saved there. It is not always possible to do what the doctor knows and is capable of doing, because sometimes the patient simply cannot arrive in time. Here, the “golden hour” can turn into days of waiting, while telemedicine becomes a temporary bridge between the battlefield and the physician. But it is here that the most important thing becomes visible: Ukrainian military medicine is not simply reacting to war — it is learning, adapting, creating new practices, and trying to turn the experience of every injury into knowledge that will help save the next patient.
And perhaps the most accurate way to describe the work of a stabilization point is not through heroic language, but in very practical terms: it is a place where people are given a chance to reach the next opportunity. To the hospital. To surgery. To a prosthetic. To rehabilitation. To life after injury.
That is why the main question for this system is not only how many medics work at stabilization points or what equipment they have. The main question is how to ensure that wounded soldiers reach them sooner, how to give doctors more time, how to make telemedicine systematic, how to make training continuous, and how to ensure that frontline experience is not lost in isolated stories, but transformed into standards.
Because in war, medicine often begins not when the patient reaches the operating table. It begins much earlier — at the moment when someone manages to bring them out alive.